INTRODUCTION TO COVID-19
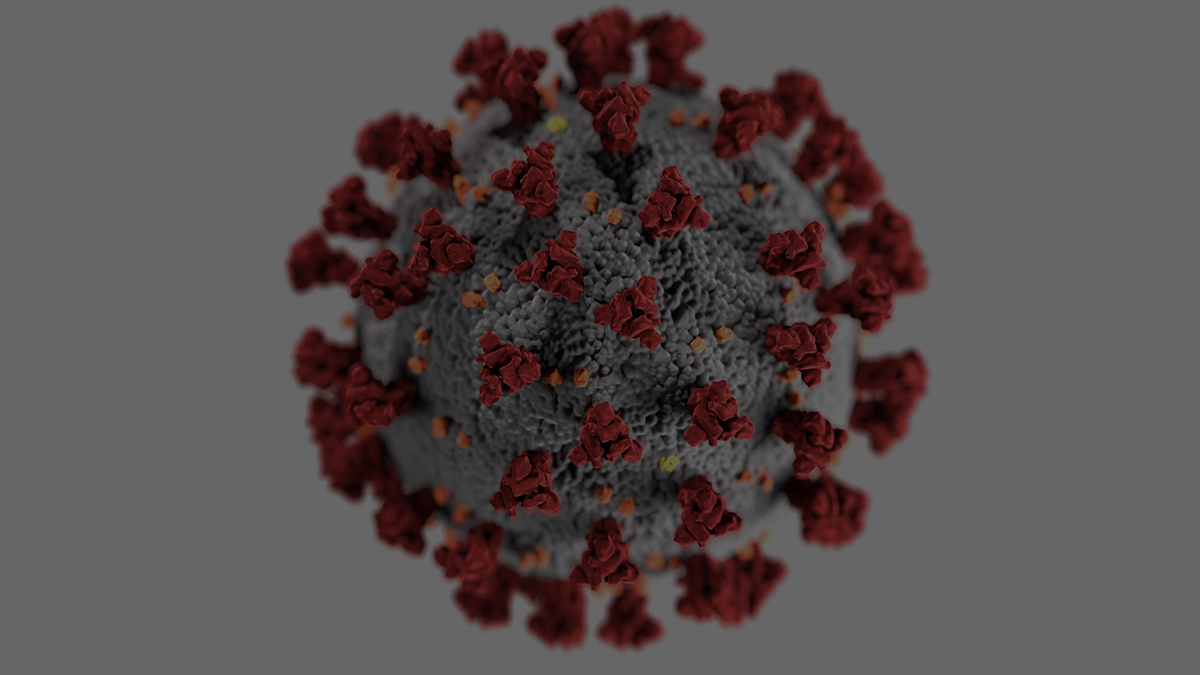
Coronavirus Disease 2019 (COVID-19) is an infectious disease caused by a virus referred to as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that was first identified in November 2019 in Wuhan, China.
This virus is new and is referred to as “novel” because it has never infected the human body before.
Common symptom presentations include flu-like symptoms, fever, cough, and shortness of breath.
Non-respiratory symptoms can include nausea, diarrhea, muscle pain, loss of smell, and headache.
The virus is spread via respiratory droplets and from touching contaminated surfaces and transferring it to eyes, nose, and mouth, usually from hands. (1, 2)
“The beginning of health is to know the disease.”
– Miguel de Cervantes
A virus is an intracellular parasite on the human cell, completely inert until it penetrates its victim’s cellular membrane. A viral surface protein must perfectly and exactly “dock” onto the human cell membrane in order for it to inject its RNA (information) for transcription (replication) to occur.
The infected cell will burst and release the now multiplied virus and the process starts over again with even more viruses to potentially infect more cells. (3)
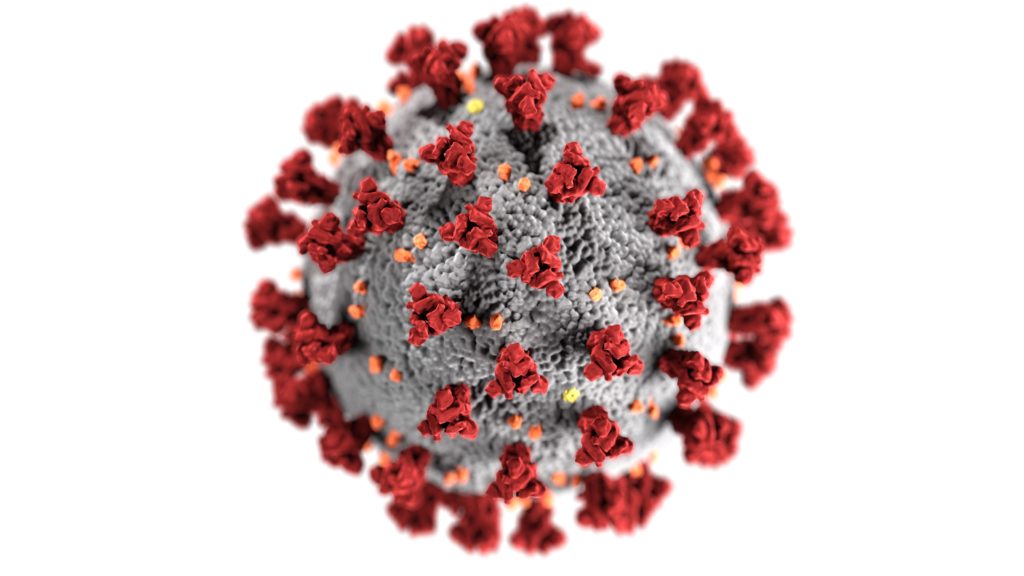 COVID-19 has a distinctive spike protein that is able to bind to the human cell by angiotensin-converting enzyme 2 (ACE2) and enter the cell. ACE2 is found on the outer surface lining of type II alveolar cells of the lungs but also in the kidney, heart, arteries, and gastrointestinal tissue; this virus cannot attack tissue that does not contain ACE2.
COVID-19 has a distinctive spike protein that is able to bind to the human cell by angiotensin-converting enzyme 2 (ACE2) and enter the cell. ACE2 is found on the outer surface lining of type II alveolar cells of the lungs but also in the kidney, heart, arteries, and gastrointestinal tissue; this virus cannot attack tissue that does not contain ACE2.
“The microbe is nothing, the terrain is everything.”
– Louis Pasteur
These are the last words spoken by Louis Pasteur, Father of the Germ Theory, recanting his famous theory that microbes cause disease and aligning with Antoine Bechamp who believed disease was a condition of imbalance in the internal terrain of the body.
In the Terrain theory, if you elevate the health of the host, the internal resistance prevents the virus from being able to invade the cell and replicate, and prevent the disease from ever occurring.
The Virus Host Interaction
This virus-host interaction seems to determine disease state. If the virus cannot enter the cell it cannot become active, and therefore cannot infect the cell and cause sickness. Antonine Bechamp’s Terrain Theory explains the wide range of outcomes when testing positive for COVID-19 and also why the majority of severe cases also have a coinciding chronic health condition.
The grand majority, 81%, of positive COVID-19 cases present with mild symptoms that can be self-managed at home.
A positive COVID-19 case can even be completely asymptomatic, though the exact percentage is unknown.
The potential for the infection to suddenly turn severe is the real cause for alarm.
Interactive graph updated in real time
Severe Cases
The severe cases of COVID-19 are the minority but end up requiring urgent and often extreme life saving measures.
The body’s own natural immune defense against the virus is what ultimately causes the patient’s critical state and for some their ultimate demise.
The more aggressively the virus can reproduce within the host cell, and spreads to new cells, the more rapidly it takes over the host.
The immune system has no choice but to respond with equal aggression, causing the air sacs in the lungs to become inflamed and filled with fluid causing pneumonia.
At this point, gas-exchange can no longer happen the patient’s ultimate fate is acute respiratory distress (ARS) and shock.
This massive and exaggerated immune response is called a cytokine storm. This is the tipping point of no return for most cases and is heavily influenced by pro-inflammatory interleukin 6 (IL-6) which is like an immune soldier firing in all directions.
If patients prior to COVID-19 infection have an already heightened IL-6 inflammatory response, this puts them in much greater risk of creating a cytokine storm response.
This would be the case in most infectious diseases, patients who have cardiovascular disease, diabetes, autoimmune disease, asthma, schizophrenia, depression, and other inflammatory driven diseases.
Cytokine storm can be measured with a simple serum ferritin blood test.
 Immunosuppressant drugs may have benefit in late-stage COVID-19 by slowing down the exaggerated immune response, preventing fatal ARS. The patient will still have the viral infection, but their lung function could be preserved.
Immunosuppressant drugs may have benefit in late-stage COVID-19 by slowing down the exaggerated immune response, preventing fatal ARS. The patient will still have the viral infection, but their lung function could be preserved.
It is unknown at this time if hydroxychloroquine can exhibit any antiviral effect on SARS-CoV-2. Antibiotics may lessen the cytokine reaction likely due to a secondary bacterial infection that may happen during late stage COVID-19.
Now that foundational knowledge is established on COVID-19, this article will expand on prevention, chronic conditions that increase mortality rate of COVID-19, the relevance of a healthy gastrointestinal tract, relevant essential micronutrients, and various other discussion worthy considerations in managing COVID-19.
PREVENTION
The unseen nature of SARS-CoV-2 and its potential two-week incubation period has seemingly stopped the world from turning in the wake of this global pandemic.
Avoiding exposure to SARS-CoV-2 is the best way to prevent COVID-19.
“An ounce of prevention is worth a pound of cure”
– Benjamin Franklin
Great efforts are being made to reduce the spread of disease by following strict hygienic practices, social distancing, and shelter in place orders. (1, 2)
How SARS-CoV-2 is Spread:
- SARS-CoV-2 is spread through respiratory droplets.
- It is also spread by touching surfaces that have those droplets and introducing them into your system via mouth, nose, and eyes.
- Coughing and sneezing into a tissue or into an elbow is best practice to prevent the wide spread of respiratory droplets potentially containing the virus. (1, 2)
 During a global pandemic, washing your hands frequently is the cheapest and most important way to prevent the spread of a virus. (4)
During a global pandemic, washing your hands frequently is the cheapest and most important way to prevent the spread of a virus. (4)
The SARS-CoV-2 virus is surrounded by a lipid bilayer envelope. This lipid lining will degrade and subsequently dismantle the virus when washing your hands for 20-30 seconds with soap and warm water.
It is crucial that hands are wet with warm running water, enough soap is used to cover the hands, and that all surfaces are scrubbed including the back of hands, between fingers, and under nails.
Rinsing thoroughly and drying with a clean towel is essential to completing this cleansing process. (4)
The practice of quarantine began in the fourteenth century in response to the Black Death. (5)
Quarantine and social distancing was utilized during the 1918 influenza pandemic and reduced spread and mortality rates.

Social distancing works best when implemented in the early stages of the pandemic to reduce widespread disease transmission.
Travel restrictions are effective due to the asymptomatic carrier state and a long incubation period. (5)
R0 (pronounced “R naught”) is the mathematical measure of how contagious an infectious disease is. If the R0 of 1 that means one infected person will spread the disease and infect one other person.
The R0 value of SARS-CoV-2 is an R0 of 2-5, meaning every infected person will spread the virus to 2-5 other humans, who will then infect another 2-5 humans, and so on exponentially. (6)
For comparison, the 1918 influenza pandemic had an R0 of 1.8, a much smaller ability to spread. (7)
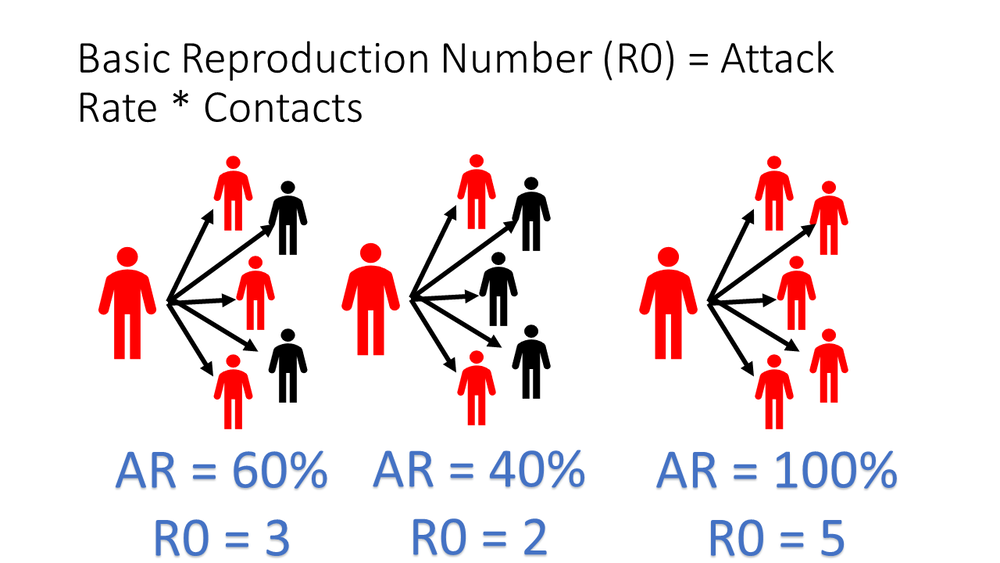
The Diamond Princess cruise line has offered a miniature epidemiological study to best understand COVID-19. Prior to cabin quarantine, the R0 value was an R0 of 7, a high volume likely due to the confined nature of a sea vessel. Once cabin quarantine was in place this number dropped to an R0 of >1, which, in theory, is low enough for the disease to eventually die out. (8)
Preventing exposure to the virus altogether is the best way to prevent COVID-19.
But what happens if you are exposed?
Why do some positive cases remain asymptomatic or only report mild symptoms?
An existing chronic condition seems to be a large risk factor determining the outcome.
CHRONIC CONDITIONS RISK FACTOR
Germ Theory
If Pasteur’s Germ Theory was completely accurate, a microbe would define outcome with universal results. One germ, one disease. No other factors would be involved when confronted with a microbe. This simply cannot be true.
The vast differences in COVID-19 range from completely asymptomatic to death. If the germ does not define the outcome, could the health of the host be the determining factor?
Host Health
Bechamp’s Terrain Theory focuses on the biology of the host, instead of the microbe. One thing is certain through all the unknowns and conflicting thoughts-outcome is gravely influenced by the patient’s very own inflammation and oxidation status. Basically the fire and rust in the body.
The most common risk factor in severe COVID-19 is the existence of a chronic condition.
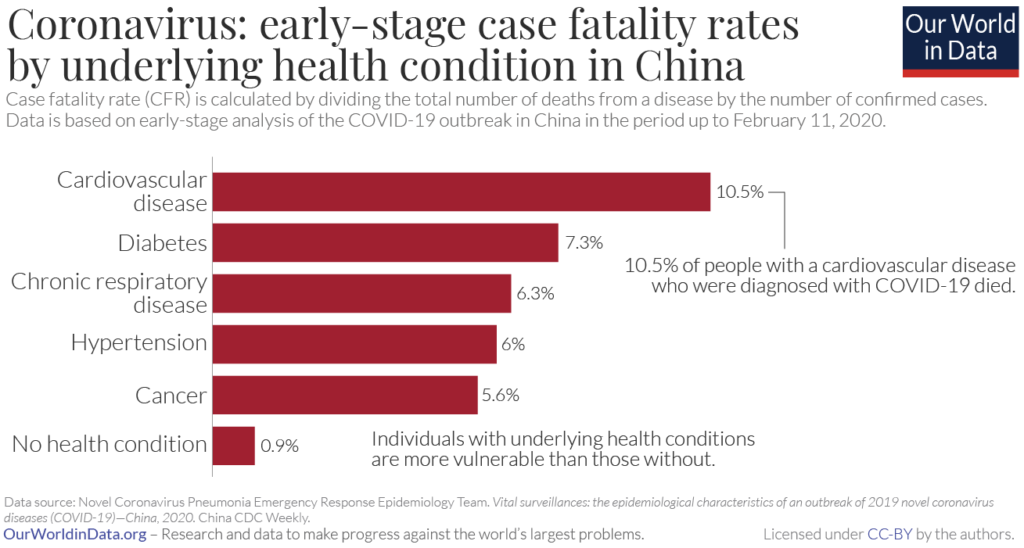
Per CDC reporting the majority of COVID-19 deaths have occurred among patients with underlying health conditions, particularly cardiovascular disease, diabetes, respiratory disease, hypertension, and cancer are the most common preexisting conditions associated with death from COVID-19.
Fire and Rust
Nearly all cardiovascular conditions are rooted in uncontrolled inflammation and oxidation. A truly deadly combination as cardiovascular disease is the number one killer in the United States. Cardiovascular diseases like hypertension and arteriosclerosis are slow and silent killers taking decades to manifest into its end stage of disease. The patients who have cardiovascular disease have a pro-inflammatory loaded gun when faced with COVID-19. Their scale is already weighted and the viral cascade can be the tipping point of no return. (10)
Diabetes
Diabetes is the second most common comorbidity risk factor and often times doubles down by coexisting with cardiovascular disease. The diabetic state impairs cytokine response and T-cell activation. Activated innate immune cells in metabolic tissue lead to the release of inflammatory mediators which promotes systemic insulin resistance. Diabetes is a condition of sugar dysregulation and sugar is not only inflammatory but down regulates the immune system.
Immunocompromised
Any condition that is rooted in a dysfunctional immune system, like cancer and autoimmune conditions, will be risk factors for contracting SARS-CoV-2 and having COVID-19 complications. The battle against the foreign invader and appropriate response once infected is a delicate balance that is unlikely to favor a patient who is immunocompromised.
Addressing and managing your preexisting chronic condition may be the most effective route for preventing SARS-CoV-2 infection and preventing severe COVID-19.
GASTROINTESTINAL HEALTH CONNECTION
“All diseases begin in the gut.”
– Hippocrates
Your microbiota is considered its own organ system and is a collection of trillion of cells in and on your body. We have a critical symbiotic relationship with our microbiota as it provides many key mechanisms but notable in this context it modulates our immune system. The balance of friendly bacteria within the gastrointestinal system can determine one’s health status.
Certain floral patterns can predict disease and some illnesses can be resolved by simply rebalancing the flora. Dysbiosis is a term used to describe an imbalance in the gut. A simple stool test can be ordered that profiles the “residents” in your gastrointestinal tract as well as the short chain fatty acids needed to support them. The delicate balance of bacteria can be greatly compromised by multiple factors including but not limited to ubiquitous levels of Glyphosate (Roundup), overuse of antibiotics, a diet high in refined carbs and low in vegetable fiber, and other lifestyle habits.
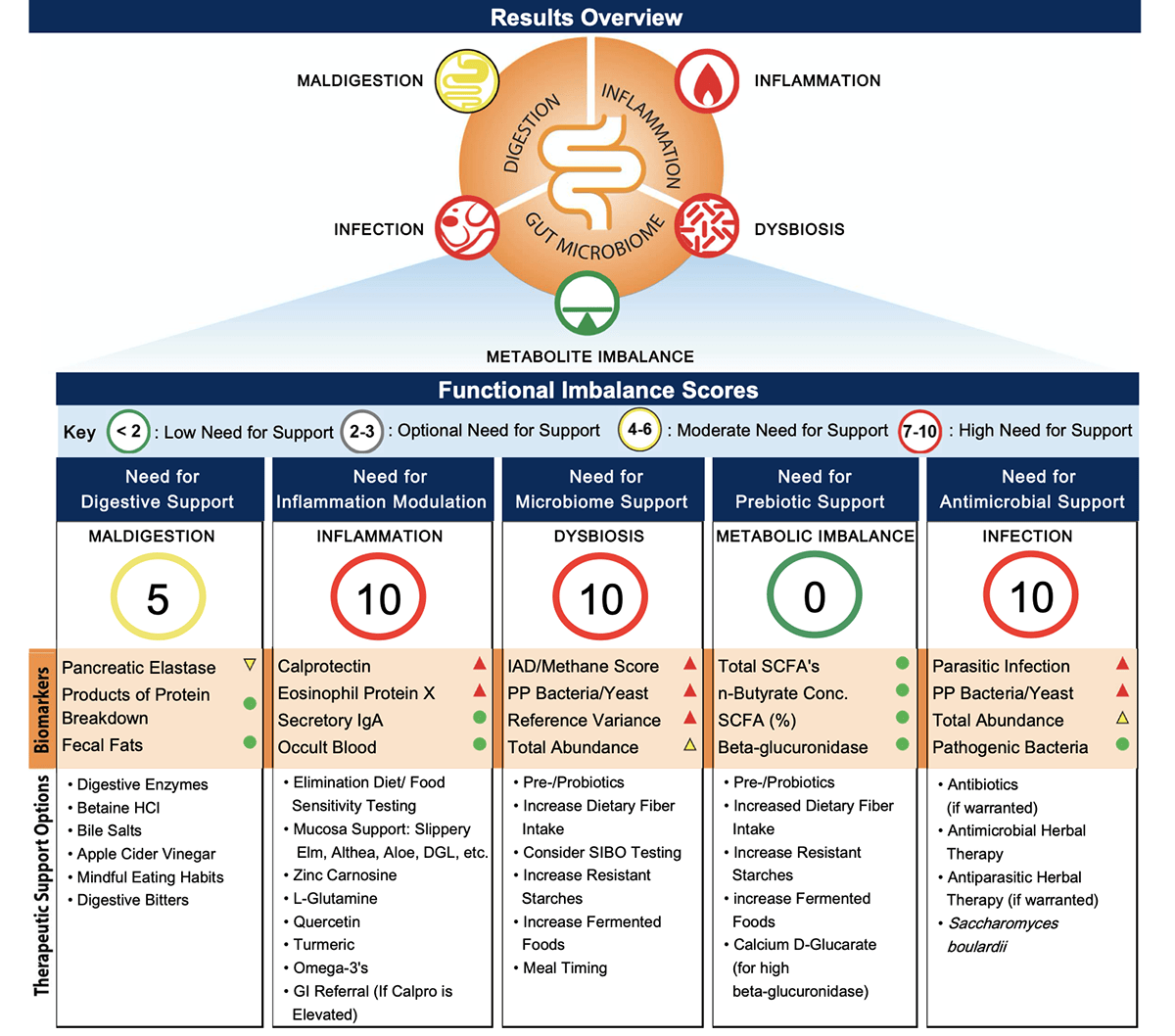
Genova Labs GI Effects Stool Test
A diverse microbiome is desired in a healthy gastrointestinal tract with Lactobacillus and Bifidobacterium being the predominant strains. In Zhejiang Province, patients who had COVID-19 concurrently had decreased levels of these microbes. (10) They also had secondary fungal infections which is presumed to be opportunistic and can be prevented and managed with the administration of appropriate probiotics. These findings were significant enough for the First Affiliated Hospital of Zhejiang University School of Medicine to recommend assessment of gastrointestinal function for all patients. (10)
Gastrointestinal complaints, such as diarrhea, have been reported with COVID-19 infection. The American Journal of Gastroenterology reports a subgroup of positive COVID-19 patents who have digestive symptoms as their only symptom without any respiratory manifestation. It is believed to be due to the ACE2 expression found on upper and lower gastrointestinal tract tissue to be100-fold higher than in respiratory organs. This means the COVID-19 virus can dock on gastrointestinal lining 100x more easily than respiratory tissue. Over half of COVID-19 infected patients tested positive for its viral nucleic acid in their feces. More curious, nearly a quarter of cases studied had negative respiratory samples but positive stool samples. (11)
Metabolites of gut microbes modulate the immune system of distal organs like the lung. The bi-directional cross-talk between gut and lung (gut-lung axis) flora have been linked with exacerbations in chronic lung disorders and patients acutely infected with the coronavirus. Virus infected individuals generally present an increased prevalence of Haemophilus and Moraxella in the gut and these unsavory bacteria strongly compete for the same habitat against friendly flora Lactobacilli. (13). These microbiome shifts are not due to active infection in the gut but do lead to immune injury and inflammation that is likely the tipping point in severe COVID-19 cases.
The mechanism in which COVID-19 is able to enter the gastrointestinal tract is unknown at this time. It is a worthy discussion in regards to communities of high risk individuals like nursing facilities where fecal-oral transmission of disease is common. Failure to recognize symptoms lead to exponential spread of disease from those who remain unaware and undiagnosed. Further understanding of this mechanism will shed light on diagnosing and perhaps prevention of COVID-19.
MICRONUTRIENTS RELEVANT TO COVID-19
“Provided one has the correct level of vitamin, mineral, and nutritional input, the body can overcome disease.”
– Linus Pauling
Since SARS-CoV-2 is a novel virus, the body is relying on its innate immune system as its only line of defense. There are no antibodies trained to fight this virus at this primary stage of exposure because the body has not been previously exposed. The innate immune system has physical (mucosal barriers), chemical (cytokines), and immune cells (NK cells). These defenses and defenders need to be built and mediated to our benefit. (3). Immunity status after exposure to SARS-CoV-2 is not completely known but antibody testing is hopeful in proving immunity status, though the length of immunity after exposure is unknown.
The average American is deficient in vital micronutrients needed for essential life functions for reasons beyond this subject. The high metabolic need required to ward off a novel virus utilizes above average nutrient supply. Having adequate micronutrients will facilitate this divine process. A micronutrient lab panel can be ordered, evaluated, and managed accordingly by a licensed healthcare provider trained in optimal parameters. Naturally, all micronutrients are fundamental; but the following are especially necessary to support the challenged innate immune response when exposed to SARS-CoV-2.
Micronutrient Test From Genova Labs
Vitamin D
Vitamin D is known as the “sunshine vitamin.” Patients with respiratory disease are frequently deficient in Vitamin D. The majority of the population do not have ideal levels between 50-80mg/mL. Vitamin D stimulates NK cells of the innate immune system whose job is to neutralize the virus upon entry into the body before it even has a chance to invade the cell. Vitamin D favorably influences pro inflammatory cytokines. (14, 16, 17,19)
Acute Respiratory Distress Syndrome (ARDS) is the deadly condition that occurs in late stage COVID-19. The frequency of ARDS due to COVID-19 surpasses the nation’s supply of ventilators necessary to save the live’s of all who need respiratory support. In a profound study, 90% of ARDS patients were deficient in vitamin D, which they defined as under 20mg/mL, and low vitamin D was associated with longer duration of mechanical ventilation. (15) In these cases, properly supplemented vitamin D levels could be the difference between life and death and could potentially reduce the overwhelming need for ventilators nationwide.
Vitamin C
Vitamin C functions as an antioxidant, essential for collagen production, supports the innate immune system, and is anti-viral. Humans are unable to make vitamin C and it not stored in tissue, so a daily diet rich in vegetables and fruits is essential to life. Vitamin C is showing positive results in clinical trials that began in February 2020 in China utilizing Vitamin C infusions for late stage COVID-19 severe acute respiratory infection. Doctors hypothesize Vitamin C can help improve prognosis measured by decreased mortality, ventilation-free days, less first aid measures, respiratory indexes, and ventilator parameters. (16,17,20)
Zinc
Zinc is a mineral used to support barriers (lung and gut lining) and has a direct antiviral effect against some viruses. In past studies on SARS-coronavirus, zinc has been shown to inhibit RNA replication. So if the virus docks onto the ACE2 of the cell and injects its RNA into the cell, zinc may prevent it from multiplying and being able to exponentially spread to other cells. Zinc also has anti-oxidant and anti-inflammatory effects. Symptoms of zinc deficiency include loss of smell and taste, pica, depression, alopecia, and impaired wound healing. (16,17,18)
Vitamin A
Vitamin A plays a role in maintaining barrier lining like the respiratory and gastrointestinal tract and serves as an antioxidant and anti-inflammatory. It especially supports the mucus-secreting cells that physically “trap” pathogens attempting to invade the body. Vitamin A modulates T helper immune cells that influence cytokines. Vitamin A is rich in carotenoids like carrots and pumpkins, liver oils, dark leafy greens, and eggs. Vitamin A supplementation dose should be closely monitored by a healthcare professional due to toxicity concerns. (16,17)
Vitamin E
Vitamin E is a known antioxidant which is important in the lung to clear free radicals that trigger cytokine response, potentially preventing the late state cytokine storm. Vitamin E is high in sunflower seeds, almonds, avocados, and leafy greens. Supplementation of Vitamin E requires knowledge of alpha-, gamma-, delta-, gamma-tocopherols and avoidance of its commonly used synthetic form.
Selenium
An important antioxidant like NAC is selenium, a cofactor for glutathione peroxidase and a key nutrient for the immune system. Due to deficient levels in the soil, the American diet tends to be insufficient in selenium. Brazil nuts are known for being rich in selenium. It is important to have this evaluated by a health professional as iodine, zinc, and copper levels influence necessity. (16)
N-Acetyl-Cysteine
N-acetyl-cysteine (NAC) is a precursor to the body’s master antioxidant, glutathione. NAC is a mucolytic, meaning it is able to break down mucus in the upper respiratory tract which causes coughing, the hallmark symptom of COVID-19. NAC is required for the body’s repair mechanisms in response to disease. Severity of disease can be determined by the body’s ability to keep up with viral destruction. (16)
Glutathione
Glutathione is the body’s master antioxidant. It’s importance in the body cannot be overstated as it directly and instantly neutralizes oxidative stress (rust). Oxidative stress plays a central role in viral replication and the immune system’s exaggerated cytokine inflammatory response. Antioxidants counter this stress and protect human tissue from being an innocent bystander in the immune system’s war against invaders. Glutathione is friendly to fellow antioxidants by recycling Vitamin C and Vitamin E. Lung glutathione metabolism is widely recognized as a central feature of many severe inflammatory lung conditions including acute respiratory distress syndrome. (32)
Omega Fatty Acids
Inflammation response is greatly influenced by omega-3 fatty acids status and its relation to omega-6 fatty acids. These essential fatty acids serve many foundational purposes. Nearly every cell in your body is lined with two layers of fat. The types of fats consumed determine the type of fats that line the cell. You literally are what you eat!
Omega fatty acids are responsible for the synthesis of prostaglandins and leukotrienes that can influence pain and inflammation. Eicosapentaenoic acid (EPA) is known for its anti-inflammatory ability because of its alternate pathway away from inflammation inducing arachidonic acid (AA). Omega-6 fatty acids can be pro-inflammatory and are overly consumed in the standard American diet presumed to be due to excessive use of corn oil and grain fed animal protein. The omega-6 to omega-3 ratio can be used as a measurement of cellular inflammation. A diet rich in wild caught fish, seeds, and nuts will provide omega 3 fatty acids. (16)
Potassium
Potassium plays an interesting role in COVID-19. Sodium and potassium are exchanged at the ACE2 on the cell. Once the virus has attached onto the ACE2, sodium and potassium can no longer be exchanged. In China, 93% of critically ill patients had low potassium. These patients responded well when given supplementation to correct the deficiency. It is unlikely that potassium is a preventive therapy, but a consideration upon infection that plays a role in treatment outcome. (21)
Deficiencies or insufficient micronutrients can be due to lifestyle, genetics, medication, or disease state. Each micronutrient has many different chemical forms that are specific to function. It is important to have a professional evaluation of history, a review of systems, physical examination, and laboratory values prior to starting any nutritional supplement protocol.
THERAPEUTIC CONSIDERATIONS
Fight fire with fire
A social media post gave undue concern about using steroids (cortisone) and non-steroidal anti-inflammatory drugs (ibuprofen) during a COVID-19 infection. Experts agree, there is no scientific evidence to support consuming these drugs would cause an increased risk or progress the disease. On the contrary, an elevated body temperature plays a major role in defense by directly inactivating the virus particles, particularly in enveloped viruses like COVID-19, and may reduce replication rate. When infected with a novel virus, your body’s innate immune system will trigger a fever to kill the pathogen. Fevers are the most common reason for an unscheduled primary care visit in the pediatric population. All pathogens are new to their immature immune system and they rely heavily on their innate system for battle. After the battle, antibodies are formed and a more precise battle can be fought in the future. This is why children have more fevers than adults and “fever phobia” is documented as such in the literature. Per the World Journal of Clinical Pediatrics, a “moderate fever” below 104°F is beneficial and the principle benefit of an antipyretic drug (fever reducer) is to “make children more comfortable and to relieve the parents’ anxiety.” The high metabolic demand of fever requires adequate hydration and electrolyte replacement. (1,3,23,24,25)
Quercetin
Quercetin is a polyphenol derived from plants like leafy vegetables, broccoli, red onions, apples, and tea that is often used to stabilize the mast cell and prevent histamine release. It serves as an anti-oxidant and modulates the inflammasome response that causes the cytokine storm and has post-viral healing. Most notable is its antiviral capability against SARS-CoV. (27)
Resveratrol
Resveratrol is also a naturally occurring polyphenol found in plants and it’s purpose is to protect the plant from pathogens. It is found in many functional foods like grapes, blueberries, and cocoa. It is a potent inhibitor of the inflammasome responsible for the cytokine storm. A promising study showed it can inhibit SARS-CoV2’s virus cousin, MERS-CoV. (26)
Curcumin
Curcumin, the main ingredient in turmeric, is a potent anti-inflammatory, a very strong anti-oxidant, and offers anti-microbial protection. Turmeric is also a powerful pain reducer. It is a spice derived from a root commonly used in food. As previously explained, controlling the fire is paramount in COVID-19 survival. (25,26,27)
Elderberry
Elderberry (Sambucus nigra) has a long history worldwide across many cultures for immune support. It is antiviral, can inhibit viral replication, and can aid the defense/repair mechanism often compromised with viral assault. It contains flavonoids like quercetin and anthocyanidins and has a deep purple color with a delightful taste. The medicinal syrup can be homemade with freshly grown elderberries but use great caution due to potential cyanide buildup if not prepared properly. (30)
Monolaurin
Monolaurin is lauric acid derived from coconut oil and has the ability to kill the virus by dissolving its lipid envelope, similar to what happens to the virus when you wash your hands with soap. It is known to inactivate viruses by binding to their lipid envelope and preventing it from ever attaching to the human cell, leaving the virus completely inactive and unable to infect the cell and replicate. It is deemed GRAS by the FDA and sold as a dietary supplement since it is virtually impossible to get the therapeutic dose of monolaurin through coconut oil consumption. (31)
Melatonin
Children are seemingly spared from COVID-19 although they can be asymptomatic carriers. One theory credits higher levels of melatonin in childhood that decrease in older age. Melatonin is anti-viral, anti-inflammatory, and has immunosupportive qualities. You can optimize your melatonin levels naturally by practicing a healthy sleep-wake cycle, spending time in natural sunlight for twenty minutes in the morning, wearing blue light filter glasses, honoring a “digital sunset” in the evening, and managing stress levels. Elevated cortisol levels will decrease melatonin levels. Melatonin can be supplemented prior to bedtime under the supervision of a licensed professional. (17)
FINAL THOUGHTS
Elevating the health of the host is the best practice when fighting against a novel virus.
Supporting the innate immune system, facilitating a precise adaptive response, and reducing post-war cleanup by protecting barrier tissue determines the state of disease.
Should the focus be solely on the virus? Absolutely not.
If the host defenses and defenders are adequately reinforced, they can protect the human body from all pathogens trying to invade and destroy.
This can be accomplished by managing a preexisting chronic condition, maintaining gastrointestinal health, balancing micronutrients, and utilizing natural treatment considerations.
To have your health evaluated by a licensed physician, click here to become a patient.
Authored by: Dr. Brittany Parisot-Sebby

Disclaimer: This article was released April 9th, 2020 and reflective of the currently limited science specific to COVID-19. Clinical assumptions are being made worldwide to manage this global crisis and pandemic.
This article is written based on current literature published on COVID-19, accepted basic human physiology, immunology, and clinical nutrition.
This article is referenced and presents information that is in no way intended to diagnose or treat any condition. To have your health evaluated and managed by a licensed professional, please click here to become a patient.
Sources:
- https://www.who.int searched 29 March 2020.
- https://www.cdc.gov searched 29 March 2020.
- Levingson, Warren. Review of Medical Microbiology and Immunology, 10th ed. McGraw Hill. 2008.
- https://www.unicef.org searched 29 March 2020
- Nita Madhav, Ben Oppenheim, Mark Gallivan, Prime Mulembakani, Edward Rubin, and Nathan Wolfe. Disease Control Priorities: Improving Health and Reducing Poverty. 3rd Edition. Chapter 17: Pandemics: Risks, Impacts, and Mitigation.
- Yixuan Wang Yuyi Wang Yan Chen Qingsong Qin. “Unique Epidemiological and Clinical Features of the Emerging 2019 novel coronavirus pneumonia (COVID-19) Implicate Special Control Measures.” Journal of Medical Virology. 5 March 2020.
- Biggerstaff M, Cauchemez S, Reed C, Gambhir M, Finelli L. “Estimates of the Reproduction Number for Seasonal, Pandemic, and Zoonotic Influenza: A Systematic Review of Literature.” BMC Infectious Disease. 04 September 2014.
- Mizumoto, K., Kagaya, K., Zarebski, A. & Chowell, G. “Estimating the asymptomatic proportions of coronavirus disease 2019 (COVID-19) cases on board the Diamond Pincess cruise ship.” Yokohama, Japan, 2020. Euro Surveill. 25, 2000180 (2020).
- Jing Yang, Ya Zheng, et al. “Prevalence of Comorbidities in the Novel Wuhan Coronavirus (COVID-19) Infection: A Systematic Review and Meta-Analysis.” International Journal of Infectious Disease. 5 March 2020.
- Xu K, Cai H, Shen Y, et al. 2020;49(1):0. “Management of Corona Virus disease-19: The Zhejiang Experience.”
- Chaoqun Han, et al. “Digestive Symptoms in COVID-19 Patients with Mild Disease Severity: Clinical Presentation, Stool Viral RNA Testing, and Outcomes.” American Journal of Gastroenterology. Prepublished March 2020.
- Gu J, Han B, Wang J. COVID-19. “Gastrointestinal manifestations and potential fecal-oral transmission.” Gastroenterology 2020.
- Anand S, Mande SS. “Diet, Microbiota, and Gut-Lung Connection.” Frontiers in Microbiology. 2018; 9:2147. Published 2018 Sept 19.
- Marsland, B. Trompette, A. Gollwitzer, E. “The Gut-Lung Axis in Respiratory Disease.” Annals of the American Thoracic Society. 2015 March 09.
- Zdrenghea MT, Makrinioti H, Bagacean C, Bush A, Johnston SL, Stanciu LA. Vitamin D modulation of innate immune responses to respiratory viral infections. Rev Med Virol. 2017;27(1):10.1002/rmv.1909. doi:10.1002/rmv.1909
- Ednan K. Bajwa , Ishir Bhan , Sadeq Quraishi , Michael Matthay , B. T. Thompson , L. “Low Vitamin D Status Occurs in 90% of Patients with ARDS and Is Associated with Longer Duration of Mechanical Ventilation.” American Journal of Respiratory and Critical Care Medicine. 2016;193:A1846.
- Gaby, Alan. Nutritional Medicine. 2nd ed. April 2007.
- Vasquez, Alex. Antiviral Strategies and Immune Nutrition. Inflammation Mastery Series. 2014.
- Aartjan J. W. te Velthuis, Sjoerd H. E. van den Worm, Amy C. Sims, Ralph S. Baric, Eric J. Snijder, Martijn J. van Hemert. “Zn2+ Inhibits Coronavirus and Arterivirus RNA Polymerase Activity In Vitro and Zinc Ionophores Block the Replication of These Viruses in Cell Culture.”
- Grant WB, Lahore H, McDonnell SL, et al. Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients. 2020;12(4):E988. Published 2020 Apr 2. doi:10.3390/nu12040988
- ZhiYong Peng. “Vitamin C Infusion for the Treatment of Severe 2019-nCoV Infected Pneumonia.” NIH U.S. National Library of Medicine. Clinical Trial NCT04264533. 11 February 2020.
- dong chen Jr., Xiaokuni Li, qifa song Sr., Chenchan Hu Jr., Feifei Su, Jianyi Dai. “Hypokalemia and Clinical Implications in Patients with Coronavirus Disease 2019 (COVID-19).” medRxiv 2020.02.27.20028530; doi: https://doi.org/10.1101/2020.02.27.20028530
- www.aap.org. searched 8 April 2020.
- Janice E. Sullivan, Henry C. Farrar. “Fever and Antipyretic Use in Children.” Pediatrics Official Journal of the American Academy of Pediatrics. March 2011.
- Chiappini E, Bortone B, Galli L, et al Guidelines for the symptomatic management of fever in children: systematic review of the literature and quality appraisal with AGREE II BMJ Open 2017;7:e015404. doi: 10.1136/bmjopen-2016-015404
- El-Radhi AS. “Fever Management: Evidence vs Current Practice. World J Clin Pediatr. 2012; 1 (4):29-33. 2012 Dec 8. doi:10.5409/wjcp.v1.i4.29
- Lin SC, Ho CT, Chuo WH, Li S, Wang TT, Lin CC. Effective inhibition of MERS-CoV infection by resveratrol. BMC Infect Dis. 2017;17(1):144. Published 2017 Feb 13. doi:10.1186/s12879-017-2253-8
- Ryu YB, Jeong HJ, Kim JH, et al. Biflavonoids from Torreya nucifera displaying SARS-CoV 3CL(pro) inhibition. Bioorg Med Chem. 2010;18(22):7940–7947. doi:10.1016/j.bmc.2010.09.035
- Khaerunnisa S, Kurniawan H, Awaluddin R, Suhartati S, Soetjipto S. Potential inhibitor of COVID-19 main protease (Mpro) from several medicinal plant compounds by molecular docking study. Preprints. Published online March 13, 2020. doi:10.20944/preprints202003.0226.v1
- Tozser, Jozsef. “ Natural compounds as regulators of NLRP3 inflammasome-mediated IL-b production.” Mediators Inflamm. 2016;2016:5460302. doi:10.1155/2016/5460302
- Porter RS, Bode RF. A review of the antiviral properties of black elder (Sambucus nigra L.) products. Phytother Res. 2017;31(4):533-554. doi:10.1002/ptr.5782
- Thormar, H; Isaacs, C E; Brown, H R; Barshatzky, M R; Pessolano, T (1 January 1987). “Inactivation of enveloped viruses and killing of cells by fatty acids and monoglycerides”. Antimicrobial Agents and Chemotherapy. 31 (1): 27–31. doi:10.1128/aac.31.1.27. PMC 174645. PMID 3032090.
- Rahman I1, MacNee W. “Oxidative stress and regulation of glutathione in lung inflammation.” European Respiratory Journal 2000 16: 534-554









Follow Us!